
Hi, and welcome to this video on multimodal behavioral therapy!
What is the BASIC I.D. Model?
Arnold Lazarus was a South African-born clinical psychologist and researcher who coined the term “multimodal behavioral therapy”. The idea behind the term is built on the premise that we are all basic biological beings who think, smell, touch, experience emotions, and relate to others.
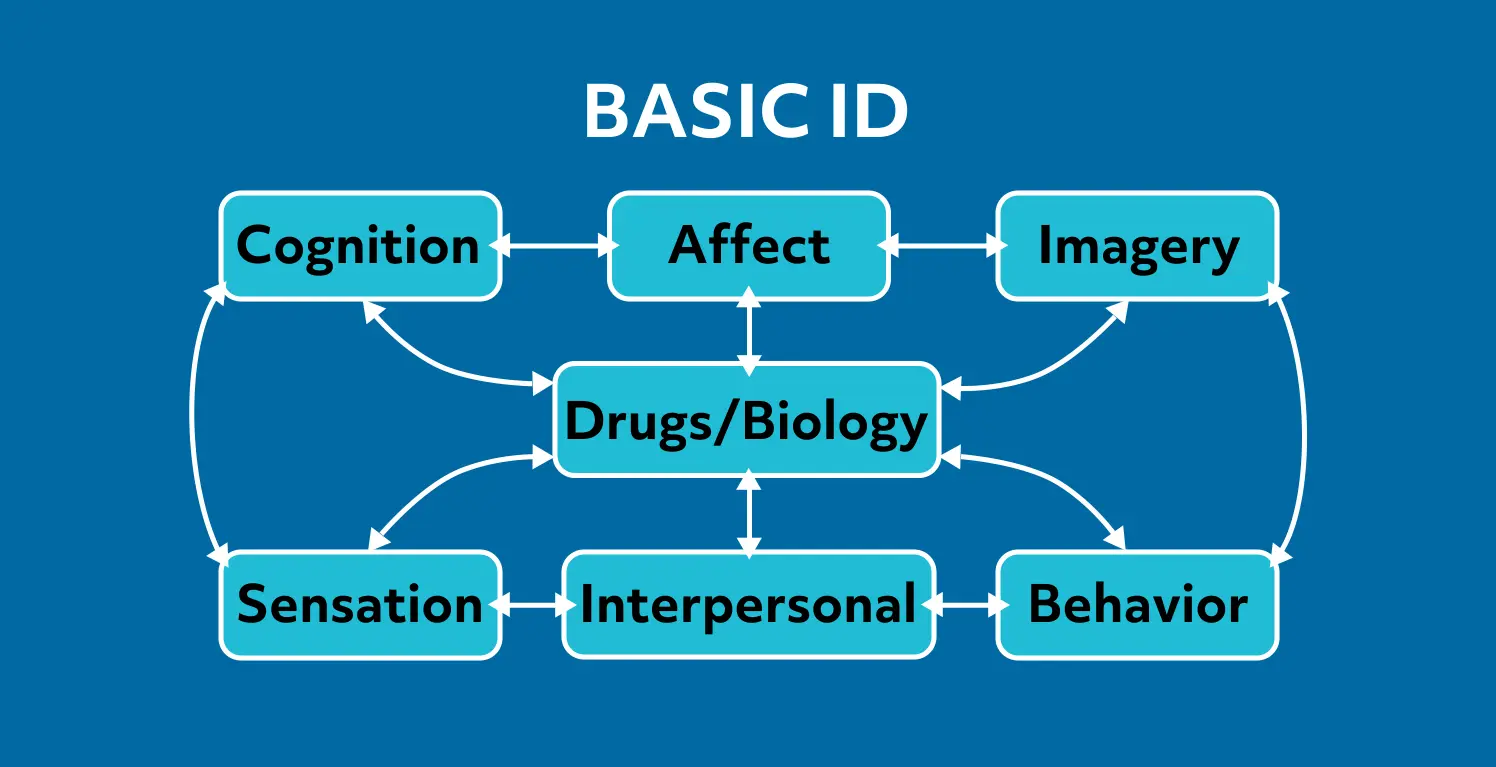
Lazarus lists the modalities in the acronym BASIC I.D.:
- Behavior
- Affect (emotions)
- Sensation (touch, smell, sight, hearing, taste)
- Imagery (thinking in pictures, self-image)
- Cognition (thinking in words, beliefs, attitudes, opinions, thinking styles)
- Interpersonal (how we relate to others)
- Drugs and biology (medications, substances, diet, exercise, general health, sleep)
Behavior
We’ll start with the first in the acronym: behavior.
Behavior is defined as the way a person acts or conducts themselves, especially as they interact with other people. To assess behavior, the clinician may ask questions such as “What is this person doing or not doing that is affecting daily living and relationships?”, “What behaviors do they need to stop or start?”, and “Are there any maladaptive behaviors, or self-defeating actions?”.
The patient may reveal these answers even as they are first meeting and speaking with the therapist, as their behaviors may be the source of discomfort or the reason they are seeking care.
Drugs and Biology
Drugs and biology must be assessed, and this area is sometimes assessed first. This assessment will take into account the patient’s health beliefs, as well as physical wellness. What do they believe about and do in regards to sleep, exercise, nutrition, weight, and alcohol and drug use, and are these habits considered “healthy” or not?
Affect
Affect can be defined as the way in which a person expresses themselves, such as “She has a sunny affect” or “His affect comes across as flat, depressed, or angry”. The clinician may assess the patient by asking themselves “What emotions are predominant?”, “What generates negative reactions?”, or “How does the person respond to questions and other interactions?”
The patient themselves may reveal during interactions what triggers certain behaviors or moods.
Sensation
Sensation can be defined as a physical feeling or perception resulting from something that happens to or comes into contact with the body. To assess sensation, see what sensations are felt or experienced when the patient is subjected to certain stimuli, noting if they have any sensory complaints. Examples might include certain sounds they cannot tolerate, like nails on a chalkboard or the creak of a slow-closing door.
Imagery
To assess imagery, ask the patient about their self-image, or if there is any imagery that is constant or that they can’t easily dismiss. This can include flashbacks and/or traumatic experiences.
Cognition
Cognition is the mental action or process of acquiring knowledge and understanding. This can be assessed by discussion of the patient’s values, beliefs, and opinions, and noting if there are any that are problematic, dysfunctional, or irrational.
Interpersonal Functioning
Interpersonal functioning is how we interact and function with others. Who are the significant others in the patient’s life? How do they interact with them? What does the patient want from relationships: what are their expectations, desires, and contributions?
Review
When a patient first presents with a complaint or a sign of distress, it will usually fall into one of these areas. This is a good starting point for clinicians to get to the root of the patient’s problem, and then the other parts of the BASIC I.D. can be brought in as the patient and the clinician develop a rapport.
Before we go, here’s a quick review question to test your knowledge:
If a patient is triggered by loud noises and begins to rock and cry, which part of the behavioral multimodal BASIC I.D. is being affected?
- Affect
- Imagery
- Cognition
- Sensation
If you chose D, sensation, you are correct!
Thanks for watching, and happy studying!
